
THERE ARE SEVERAL KEY SIGNS AND SYMPTOMS OF CTX1

CTX causes an array of clinical manifestations.1
If your patient has more than one of the below signs and symptoms, you should suspect CTX.1-5
Scroll down or click on the icon to go to a specific section

Idiopathic Bilateral Cataracts

Neurological Deterioration/ Movement Disorders

Tendon Xanthomas

Neonatal Cholestasis/ Prolonged Jaundice

Chronic Diarrhea
POTENTIAL SIGNS AND SYMPTOMS1-5

*A small number of genetic disorders affect lipoproteins and can lead to xanthomas: cerebrotendinous xanthomatosis (CTX), familial hypercholesterolemia, and sitosterolemia.6

Without early diagnosis and management, neurologic problems can progress, leading to physically disabling neurological dysfunction, psychiatric disturbances, intellectual disability, and even dementia.1,9
CTX IS CHALLENGING TO DIAGNOSE DUE TO ITS VARIABILITY AND MULTISYSTEMIC EFFECTS1
Current mean age (±SD) at diagnosis is 35.5 ± 11.8 years.1
- CTX signs and symptoms are variable in onset and severity, and not every patient experiences all clinical manifestations.1

Click here to download 2 CTX Case Studies
References:
1.
Mignarri A, Gallus GN, Dotti MT, Federico A. A suspicion index for early diagnosis and treatment of cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2014;37(3):421-429. doi:10.1007/s10545-013-9674-3
2.
Lorincz MT, Rainier S, Thomas D, Fink JK. Cerebrotendinous xanthomatosis: possible higher prevalence than previously recognized. Arch Neurol. 2005;62(9):1459-1463. doi:10.1001/archneur.62.9.1459
3.
Verrips A, van Engelen BG, Wevers RA, et al. Presence of diarrhea and absence of tendon xanthomas in patients with cerebrotendinous xanthomatosis. Arch Neurol. 2000;57(4):520-524. doi:10.1001/archneur.57.4.520
4.
Clayton PT, Verrips A, Sistermans E, Mann A, Mieli-Vergani G, Wevers R. Mutations in the sterol 27-hydroxylase gene (CYP27A) cause hepatitis of infancy as well as cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2002;25(6):501-513. doi:10.1023/a:1021211520034
5.
Verrips A, Hoefsloot LH, Steenbergen GC, et al. Clinical and molecular genetic characteristics of patients with cerebrotendinous xanthomatosis. Brain. 2000;123(Pt5)123:908-919. doi:10.1093/brain/123.5.908
6.
Federico A, Gallus GN. Cerebrotendinous Xanthomatosis. 2003 Jul 16 [Updated 2022 Mar 17]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024.
7.
Gallus GN, Dotti MT, Federico A. Clinical and molecular diagnosis of cerebrotendinous xanthomatosis with a review of the mutations in the CYP27A1 gene. Neurol Sci. 2006;27(2):143-149. doi:10.1007/s10072-006-0618-7
8.
Freedman SF, Brennand C, Chiang J, et al. Prevalence of cerebrotendinous xanthomatosis among patients diagnosed with acquired juvenile-onset idiopathic bilateral cataracts. JAMA Ophthalmol. 2019;137(11):1312-1316. doi:10.1001/jamaophthalmol.2019.3639
9.
Berginer VM, Shany S, Alkalay D, et al. Osteoporosis and increased bone fractures in cerebrotendinous xanthomatosis. Metabolism. 1993;42(1):69-74. doi:10.1016/0026-0495(93)90174-m
Idiopathic Bilateral Cataracts
IDIOPATHIC BILATERAL CATARACTS OCCUR IN MANY CASES OF CTX1,2
Approximately 85% of patients with CTX experience early cataracts in both eyes, which can appear in patients as early as childhood or infancy3
Idiopathic, or early-onset, bilateral cataracts represent a key opportunity to diagnose CTX.4
- Cataracts often present between the ages of 4 and 18 years.5,*
- Patients with juvenile-onset bilateral cataracts had up to a 500-fold higher CTX prevalence than in the general population.4
- ~2 of every 100 patients with early-onset bilateral cataracts were diagnosed with CTX.4
- Among patients with a known neurologic disorder presenting with early-onset cataracts, CTX may be the second most common cause after myotonic dystrophy.7

In CTX, cataracts are caused by a buildup of cholestanol in the lens.8
- CTX cataracts may be somewhat distinctive in their appearance or morphology.8
- The nature of the crystalline lens opacities has been described as zonular, anterior, or posterior opacities that were like spokes, dots, flecks, or snowflakes, or a combination of the above.8
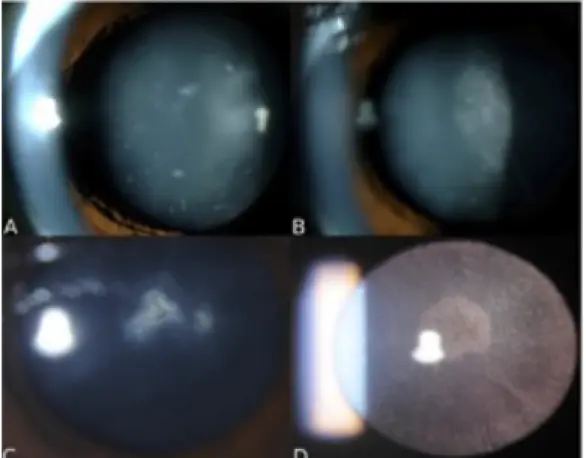
Figure reprinted from Ophthalmology, Vol. 120(5), Khan AO, Aldahmesh MA, Mohamed JY, Alkuraya FS. Juvenile cataract morphology in 3 siblings not yet diagnosed with cerebrotendinous xanthomatosis, pp. 956-960, Copyright 2013 by the American Academy of Ophthalmology, with permission from the American Academy of Ophthalmology.
Ask your patients whether cataracts without a known cause were removed early in their life.

*In CTX, cataracts usually develop in the first 3 decades of life, although a smaller number of patients develop cataracts later in life, after neurologic symptoms are already advanced.5,6
†Other causes of bilateral cataracts in children include: galactosemia,9 diabetes,10 uveitis associated with chronic juvenile arthritis,11 history of chronic corticosteroid use12 or whole body irradiation,13 hypoglycemia,14,15 or hypocalcemia.16,17
Click here for Sponsored Genetic Testing
References:
1.
Mignarri A, Gallus GN, Dotti MT, Federico A. A suspicion index for early diagnosis and treatment of cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2014;37(3):421-429. doi:10.1007/s10545-013-9674-3
2.
Verrips A, van Engelen BG, Wevers RA, et al. Presence of diarrhea and absence of tendon xanthomas in patients with cerebrotendinous xanthomatosis. Arch Neurol. 2000;57(4):520-524. doi:10.1001/archneur.57.4.520
3.
Gallus GN, Dotti MT, Federico A. Clinical and molecular diagnosis of cerebrotendinous xanthomatosis with a review of the mutations in the CYP27A1 gene. Neurol Sci. 2006;27(2):143-149. doi:10.1007/s10072-006-0618-7
4.
Freedman SF, Brennand C, Chiang J, et al. Prevalence of cerebrotendinous xanthomatosis among patients diagnosed with acquired juvenile-onset idiopathic bilateral cataracts. JAMA Ophthalmol. 2019;137(11):1312-1316. doi:10.1001/jamaophthalmol.2019.3639
5.
Verrips A, Hoefsloot LH, Steenbergen GC, et al. Clinical and molecular genetic characteristics of patients with cerebrotendinous xanthomatosis. Brain. 2000;123(Pt5)123:908-919. doi:10.1093/brain/123.5.908
6.
Dotti MT, Rufa A, Federico A. Cerebrotendinous xanthomatosis: heterogeneity of clinical phenotype with evidence of previously undescribed ophthalmological findings. J Inherit Metab Dis. 2001;24(7):696-706. doi:10.1023/a:1012981019336
7.
Cruysberg JR. Cerebrotendinous xanthomatosis: juvenile cataract and chronic diarrhea before the onset of neurologic disease. Arch Neurol. 2002;59(12):1975. doi: 10.1001/archneur.59.12.1975-a
8.
Khan AO, Aldahmesh MA, Mohamed JY, Alkuraya FS. Juvenile cataract morphology in 3 siblings not yet diagnosed with cerebrotendinous xanthomatosis. Ophthalmology. 2013;120(5):956-960. doi:10.1016/j.ophtha.2012.10.032
9.
Stambolian D. Galactose and cataract. Surv Ophthalmol. 1988;32(5):333-349. doi:10.1016/0039-6257(88)90095-1
10.
Datta V, Swift PG, Woodruff GH, Harris RF. Metabolic cataracts in newly diagnosed diabetes. Arch Dis Child. 1997;76(2):118-120. doi:10.1136/adc.76.2.118
11.
Angeles-Han S, Yeh S. Prevention and management of cataracts in children with juvenile idiopathic arthritis-associated uveitis. Curr Rheumatol Rep. 2012;14(2):142-149. doi:10.1007/s11926-011-0229-z
12.
Jobling AI, Augusteyn RC. What causes steroid cataracts? A review of steroid-induced posterior subcapsular cataracts. Clin Exp Optom. 2002;85(2):61-75. doi:10.1111/j.1444-0938.2002.tb03011.x
13.
Belkacemi Y, Labopin M, Vernant JP, et al. Cataracts after total body irradiation and bone marrow transplantation in patients with acute leukemia in complete remission: a study of the European Group for Blood and Marrow Transplantation. Int J Radiat Oncol Biol Phys. 1998;41(3):659-668. doi:10.1016/s0360-3016(98)00077-7
14.
Merin S, Crawford JS. Hypoglycemia and infantile cataract. Arch Ophthalmol. 1971;86(5):495-498. doi:10.1001/archopht.1971.01000010497002
15.
Vinding T, Nielsen NV. Two cases of acutely developed cataract in diabetes mellitus. Acta Ophthalmol (Copenh). 1984;62(3):373-377. doi:10.1111/j.1755-3768.1984.tb08417.x
16.
Hochman HI, Mejlszenkier JD. Cataracts and pseudotumor cerebri in an infant with vitamin D-deficiency rickets. J Pediatr. 1977;90(2):252-254. doi:10.1016/s0022-3476(77)80643-4
17.
Sengupta S, Ravindran RD, Kannusamy V, Tamrakar V. Bilateral simultaneous disc edema and cataract associated with Albright hereditary osteodystrophy. Middle East Afr J Ophthalmol. 2012;19(1):166-168. doi:10.4103/0974-9233.92136

Neurologic Deterioration/
CTX CAN LEAD TO SERIOUS NEUROLOGIC PROBLEMS1-3
Patients with CTX whose diagnosis is missed or delayed may face severe intellectual and physical disability.1,4
- Patients with advanced CTX show evidence of lipid deposits and loss of white matter in many areas of the brain.5,6
- Early developmental milestones may be achieved punctually, but patients then begin to fall behind.1
- Patients may exhibit poor school performance, learning difficulties, sustained infantile behavior, and lack of age-appropriate self-care skills.
- ~50% have experienced seizures.2
- ~70% have pyramidal signs, such as increased deep tendon reflexes, pathologic reflexes, and spastic paraplegia.1,4,7,8
- 60% have cerebellar signs.4
- Neurological imaging has revealed progressive unsteady paraparetic gait as a predominant symptom of adult CTX.9
- Cerebellar ataxia usually becomes evident, presenting in the second or third decade of life.1,10
Patients with CTX frequently present with movement disorders.11,12
- Gait ataxia (55%)
- Parkinsonism/parkinsonian symptoms (52%)
- Gait difficulties (38%)
- Dystonia (31%)
- Myoclonus (18%)
- Unspecified extrapyramidal symptoms (16%)
- Postural tremor (10%)
Click here for Sponsored Genetic Testing
References:
1.
Mignarri A, Gallus GN, Dotti MT, Federico A. A suspicion index for early diagnosis and treatment of cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2014;37(3):421-429. doi:10.1007/s10545-013-9674-3
2.
Gallus GN, Dotti MT, Federico A. Clinical and molecular diagnosis of cerebrotendinous xanthomatosis with a review of the mutations in the CYP27A1 gene. Neurol Sci. 2006;27(2):143-149. doi:10.1007/s10072-006-0618-7
3.
Freedman SF, Brennand C, Chiang J, et al. Prevalence of cerebrotendinous xanthomatosis among patients diagnosed with acquired juvenile-onset idiopathic bilateral cataracts. JAMA Ophthalmol. 2019;137(11):1312-1316. doi:10.1001/jamaophthalmol.2019.3639
4.
Verrips A, Hoefsloot LH, Steenbergen GC, et al. Clinical and molecular genetic characteristics of patients with cerebrotendinous xanthomatosis. Brain. 2000;123(Pt5)123:908-919. doi:10.1093/brain/123.5.908
5.
Fraidakis MJ. Psychiatric manifestations in cerebrotendinous xanthomatosis. Transl Psychiatry. 2013;3(9):e302. doi:10.1038/tp.2013.76
6.
Smithard A, Lamyman MJ, McCarthy CL, Gibbons CL, Cooke PJ, Athanasou N. Cerebrotendinous xanthomatosis presenting with bilateral Achilles tendon xanthomata. Skeletal Radiol. 2007;36(2):171-175. doi:10.1007/s00256-006-0139-8
7.
Ma C, Ren YD, Wang JC, et al. The clinical and imaging features of cerebrotendinous xanthomatosis: A case report and review of the literature. Medicine (Baltimore). 2021;100(9):e24687. doi:10.1097/MD.0000000000024687
8.
Nóbrega PR, Bernardes AM, Ribeiro RM, et al. Cerebrotendinous xanthomatosis: A practice review of pathophysiology, diagnosis, and treatment. Front Neurol. 2022;13:1049850. doi:10.3389/fneur.2022.1049850
9.
Dell'Aversano Orabona G, Dato C, Oliva M, et al. Multi-imaging study in a patient with cerebrotendinous xanthomatosis: radiology, clinic and pathology correlation of a rare condition. BJR Case Rep. 2020;6(1):20190047. doi:10.1259/bjrcr.20190047
10.
Rossi M, Cesarini M, Gatto EM, Cammarota A, Merello M. A treatable rare cause of progressive ataxia and palatal tremor. Tremor Other Hyperkinet Mov (N Y). 2018;8:538. doi:10.7916/D8X07Q2N
11.
Stelten BM. Cerebrotendious xanthomatosis: a treatable inborn error of metabolism. Dissertation. Donders series 598. Radboud University. March 13, 2023. Accessed April 19, 2024. https://repository.ubn.ru.nl/handle/2066/289601
12.
Wong JC, Walsh K, Hayden D, Eichler FS. Natural history of neurological abnormalities in cerebrotendinous xanthomatosis.J Inherit Metab Dis. 2018;41(4):647-656. doi:10.1007/s10545-018-0152-9

Tendon Xanthomas
TENDON XANTHOMAS OCCUR IN MORE THAN HALF OF CTX CASES1
Tendon xanthomas occur in CTX when foamy macrophages containing cholestanol, cholesterol, and other lipids infiltrate the tendon, disrupting collagen fibers in the connective tissue.2
- Tendon xanthomas are typically associated with lipid disorders, including sitosterolemia and familial hypercholesterolemia.1-4
- Tendon xanthomas often appear in the second decade, and most often affect the Achilles tendons.3,5

CTX should be suspected in all patients with tendon xanthomas and normal serum triglycerides and cholesterol.2
- Biochemical analysis of tendon xanthomas in patients with CTX characteristically shows high amounts of cholestanol and little cholesterol.3
- Sitosterolemia and familial hypercholesterolemia are associated with high plasma lipid levels, while in patients with CTX, plasma cholesterol and lipid levels are usually normal or near normal.1,2,6

Differential Diagnosis of Tendon Xanthomas
| Cerebrotendinous xanthomatosis | Familial hypercholesterolemia | Sitosterolemia | |
|---|---|---|---|
| Description | CTX is a rare, autosomal-recessive, lipid storage disease caused by a mutation in the CYP27A1 gene, resulting in deficiency of sterol-27-hydroxylase1,7,8 | Familial hypercholesterolemia is a group of inherited genetic defects caused by mutations in the low-density lipoprotein (LDL) receptor, apolipoprotein B (ApoB), or proprotein convertase subtilisin/kexin type 9 (PCSK9) genes that lead to the severe elevation of serum cholesterol concentration13 | Sitosterolemia is an disorder caused by mutations in ABCG5 or ABCG8 transporter genes, leading to hyperabsorption and decreased biliary excretion of non-cholesterol sterols, especially sitosterol, from the gastrointestinal tract15 |
| Diagnostic marker | Serum 5α-cholestanol9 | Serum cholesterol14 | Serum β-sitosterol16 |
| Key symptoms | Idiopathic or early-onset bilateral cataracts, neurologic deterioration/movement disorders, tendon xanthomas, neonatal cholestasis/prolonged jaundice, chronic diarrhea1,7,10-12 | Atherosclerotic cardiovascular disease, tendon xanthomas, arcus cornea (under age 45), and tuberous xanthomas or xanthelasma (under age 25)14 | Premature coronary artery disease and tendon xanthomas15 |
References:
1.
Mignarri A, Gallus GN, Dotti MT, Federico A. A suspicion index for early diagnosis and treatment of cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2014;37(3):421-429. doi:10.1007/s10545-013-9674-3
2.
Smithard A, Lamyman MJ, McCarthy CL, Gibbons CL, Cooke PJ, Athanasou N. Cerebrotendinous xanthomatosis presenting with bilateral Achilles tendon xanthomata. Skeletal Radiol. 2007;36(2):171-175. doi:10.1007/s00256-006-0139-8
3.
Rafiq M, Sharrack N, Shaw PJ, Hadjivassiliou M. A neurological rarity not to be missed: cerebrotendinous xanthomatosis. Pract Neurol. 2011;11(5):296-300. doi:10.1136/practneurol-2011-000003
4.
Melnik B. Disorders of lipid metabolism. In: Plewig G, French L, Ruzicka T, Kaufmann R, Hertl M, eds. Braun-Falco’s Dermatology. Springer, Berlin, Heidelberg. 2020. https://doi.org/10.1007/978-3-662-58713-3_89-1
5.
Moghadasian MH. Cerebrotendinous xanthomatosis: clinical course, genotypes and metabolic backgrounds. Clin Invest Med. 2004;27(1):42-50.
6.
Moghadasian MH, Salen G, Frohlich JJ, Scudamore CH. Cerebrotendinous xanthomatosis: a rare disease with diverse manifestations. Arch Neurol. 2002;59(4):527-529. doi:10.1001/archneur.59.4.527
7.
Lorincz MT, Rainier S, Thomas D, Fink JK. Cerebrotendinous xanthomatosis: possible higher prevalence than previously recognized. Arch Neurol. 2005;62(9):1459-1463. doi:10.1001/archneur.62.9.1459
8.
Stelten BML, Huidekoper HH, van de Warrenburg BPC, et al. Long-term treatment effect in cerebrotendinous xanthomatosis depends on age at treatment start. Neurology. 2019;92(2):e83-e95. doi:10.1212/WNL.0000000000006731
9.
Höflinger P, Hauser S, Yutuc E, et al. Metabolic profiling in serum, cerebrospinal fluid, and brain of patients with cerebrotendinous xanthomatosis. J Lipid Res. 2021;62:100078. doi:10.1016/j.jlr.2021.100078
10.
Verrips A, Hoefsloot LH, Steenbergen GC, et al. Clinical and molecular genetic characteristics of patients with cerebrotendinous xanthomatosis. Brain. 2000;123(Pt5)123:908-919. doi:10.1093/brain/123.5.908
11.
Verrips A, van Engelen BG, Wevers RA, et al. Presence of diarrhea and absence of tendon xanthomas in patients with cerebrotendinous xanthomatosis. Arch Neurol. 2000;57(4):520-524. doi:10.1001/archneur.57.4.520
12.
Clayton PT, Verrips A, Sistermans E, Mann A, Mieli-Vergani G, Wevers R. Mutations in the sterol 27-hydroxylase gene (CYP27A) cause hepatitis of infancy as well as cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2002;25(6):501-513. doi:10.1023/a:1021211520034
13.
De Castro-Orós I, Pocoví M, Civeira F. The genetic basis of familial hypercholesterolemia: inheritance, linkage, and mutations. Appl Clin Genet. 2010;3:53-64. doi:10.2147/tacg.s8285
14.
Bouhairie VE, Goldberg AC. Familial hypercholesterolemia. Cardiol Clin. 2015;33(2):169-179. doi:10.1016/j.ccl.2015.01.001
15.
Liebeskind A, Peterson AL, Wilson D. Sitosterolemia. In: Feingold KR, Anawalt B, Blackman MR, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; March 10, 2023.
16.
Brinton EA, Hopkins PN, Hegele RA, et al. The association between hypercholesterolemia and sitosterolemia, and report of a sitosterolemia kindred. J Clin Lipidol. 2018;12(1):152-161. doi:10.1016/j.jacl.2017.10.013

Neonatal Cholestasis/
NEONATAL CHOLESTASIS MAY BE ONE OF THE EARLIEST SIGNS OF CTX1
CTX may present as cholestatic liver disease early in the course of the disease.1
- In a retrospective evaluation of 55 patients with CTX, 8 patients (15%) had a history of unexplained neonatal cholestatic jaundice.2
- Because neonatal cholestasis in CTX may resolve spontaneously, the diagnosis may be missed.3
- However, neonatal cholestasis in CTX can be severe, resulting in liver transplant, or death.3,4

References:
1.
Clayton PT, Verrips A, Sistermans E, Mann A, Mieli-Vergani G, Wevers R. Mutations in the sterol 27-hydroxylase gene (CYP27A) cause hepatitis of infancy as well as cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2002;25(6):501-513. doi:10.1023/a:1021211520034
2.
Mignarri A, Gallus GN, Dotti MT, Federico A. A suspicion index for early diagnosis and treatment of cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2014;37(3):421-429. doi:10.1007/s10545-013-9674-3
3.
Gong JY, Setchell KDR, Zhao J, et al. Severe neonatal cholestasis in cerebrotendinous xanthomatosis: genetics, immunostaining, mass spectrometry. J Pediatr Gastroenterol Nutr. 2017;65(5):561-568. doi:10.1097/MPG.0000000000001730
4.
von Bahr S, Björkhem I, Van’t Hooft F, et al. Mutation in the sterol 27-hydroxylase gene associated with fatal cholestasis in infancy. J Pediatr Gastroenterol Nutr. 2005;40(4):481-486. doi:10.1097/01.mpg.0000150419.23031.2a
5.
Pierre G, Setchell K, Blyth J, Preece MA, Chakrapani A, McKiernan P. Prospective treatment of cerebrotendinous xanthomatosis with cholic acid therapy. J Inherit Metab Dis. 2008;31(suppl 2):S241-S245. doi:10.1007/s10545-008-0815-z

Chronic Diarrhea
CHRONIC DIARRHEA WITH INFANT ONSET IS COMMON IN CTX1
Chronic diarrhea is thought to occur in ~50% of all CTX cases.1
- In a case report and literature review, the prevalence of chronic diarrhea in patients with CTX was 65%.2
- While diarrhea is usually described as being of childhood or infant onset, it may persist into adulthood in undiagnosed patients.3
- While there are many potential causes of chronic diarrhea in children and infants, diarrhea due to CTX is thought to occur due to elevated levels of bile alcohols, which may influence gut motility, affect fluid and electrolyte transport, or affect bacterial equilibrium.3

References:
1.
Mignarri A, Gallus GN, Dotti MT, Federico A. A suspicion index for early diagnosis and treatment of cerebrotendinous xanthomatosis. J Inherit Metab Dis. 2014;37(3):421-429. doi:10.1007/s10545-013-9674-3
2.
Atallah I, Millán DS, Benoît W, Campos-Xavier B, Superti-Furga A, Tran C. Spinal cerebrotendinous xanthomatosis: A case report and literature review. Mol Genet Metab Rep. 2021;26:100719. doi:10.1016/j.ymgmr.2021.100719
3.
Verrips A, van Engelen BG, Wevers RA, et al. Presence of diarrhea and absence of tendon xanthomas in patients with cerebrotendinous xanthomatosis. Arch Neurol. 2000;57(4):520-524. doi:10.1001/archneur.57.4.520
4.
Lee KS, Kang DS, Yu J, Chang YP, Park WS. How to do in persistent diarrhea of children?: concepts and treatments of chronic diarrhea. Pediatr Gastroenterol Hepatol Nutr. 2012;15(4):229-236. doi:10.5223/pghn.2012.15.4.229
5.
Moghadasian MH. Cerebrotendinous xanthomatosis: clinical course, genotypes and metabolic backgrounds. Clin Invest Med. 2004;27(1):42-50.